SSRIs and HRV: How Antidepressants Affect Heart Rate Variability
If you start an SSRI and your wearable suddenly shows a different HRV pattern, it is easy to wonder whether the medication is helping, hurting, or confusing the signal.
The annoying truth is that all three can be possible, depending on the person. Depression and anxiety are both linked with lower heart rate variability, and antidepressants can change autonomic function too. On top of that, your sleep, symptoms, appetite, training, alcohol intake, illness, and dose timing can all move the same wearable number.
So the question is not simply, "Do SSRIs lower HRV?" The better question is: what changed, when did it change, and does the trend match how you actually feel?
Do SSRIs Affect HRV?
SSRIs may affect HRV, but the evidence is mixed and much less one-sided than it is for older tricyclic antidepressants. Some studies suggest SSRIs can reduce certain parasympathetic HRV markers, while others find little change or even small improvements after treatment. Tricyclic antidepressants show a clearer pattern of lowering HRV and raising heart rate.
That distinction matters because SSRIs are often grouped together with all antidepressants in casual wearable discussions. They should not be. Sertraline, escitalopram, fluoxetine, paroxetine, citalopram, and fluvoxamine are not the same as amitriptyline, imipramine, doxepin, venlafaxine, duloxetine, bupropion, mirtazapine, or other medications with different autonomic effects.
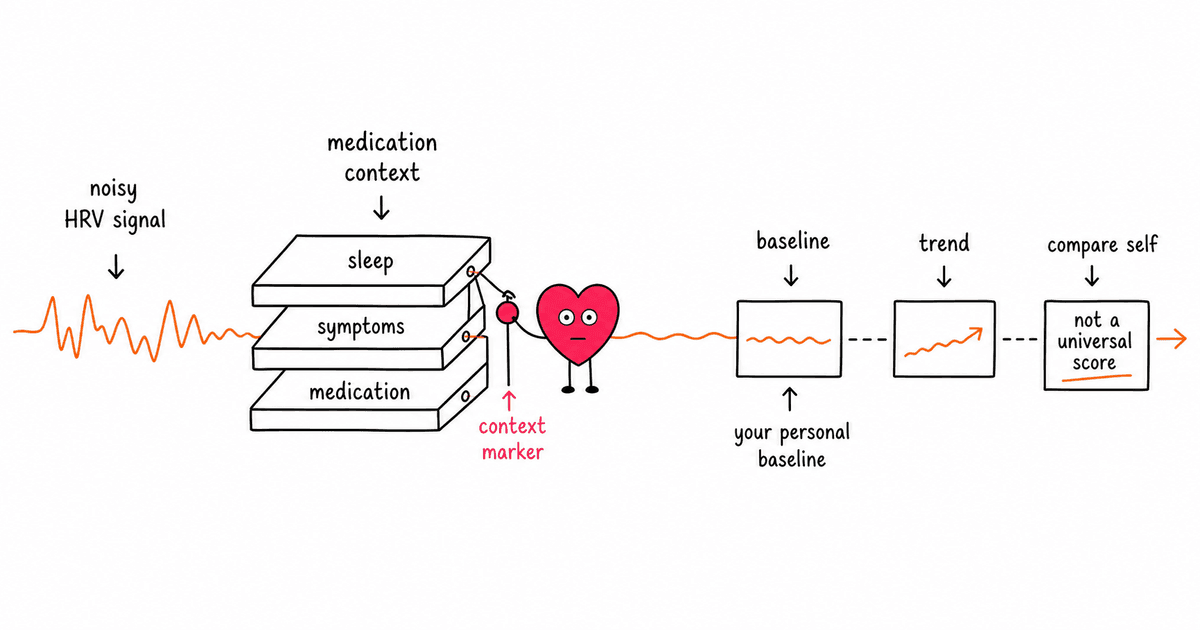
HRV is useful context. It is not a medication safety score, a mood diagnosis, or a reason to stop treatment without your clinician.
Why Antidepressants Can Change HRV
HRV reflects variation in the timing between heartbeats. Higher HRV often suggests more flexible autonomic regulation, especially stronger parasympathetic or vagal influence, but the interpretation depends on context.
Antidepressants can affect HRV through several overlapping paths.
Depression and anxiety can lower HRV before treatment starts
This is the first thing people miss.
If you started medication because of depression, anxiety, panic, chronic stress, or poor sleep, your HRV may already be suppressed before the first dose. A low baseline does not prove the medication caused the problem.
A 2010 review and meta-analysis in Biological Psychiatry found that people with major depression had lower HRV than healthy controls, and more severe depression was linked with lower HRV. That fits the broader idea that mood disorders can involve autonomic dysregulation, not just changes in thoughts or emotions.
Medication class matters
Antidepressants are not interchangeable from an HRV perspective.
SSRIs mainly target serotonin reuptake. SNRIs affect serotonin and norepinephrine. Tricyclic antidepressants can have stronger anticholinergic and cardiac conduction effects. Some medications also influence histamine, dopamine, or noradrenergic pathways.
Those differences can change heart rate, vagal tone, sweating, blood pressure, sleep architecture, and exercise response. Your wearable sees the end result, not the mechanism.
Resting heart rate can shift
HRV and resting heart rate often move in opposite directions. If a medication raises average heart rate, HRV may fall. If it lowers heart rate or improves sleep and anxiety, HRV may rise.
The tricky part is that either pattern can happen for reasons that are not obvious from the app alone. A lower HRV after starting medication might reflect a direct drug effect, but it might also reflect insomnia, nausea, appetite changes, dehydration, less activity, or a rough adjustment period.
Better mood does not always mean higher HRV right away
This is frustrating but important.
A person can feel emotionally better before HRV improves. A medication can reduce symptoms without fully normalizing autonomic patterns. Lifestyle recovery can lag behind mood recovery. If you have spent months under severe stress, your nervous system may not rebound on the same timeline as your questionnaire score.
What the Research Says
The best evidence is careful, but not perfectly clean. HRV studies vary by population, diagnosis, medication, dose, recording length, breathing control, and whether they use ECG or consumer wearables.
Depression itself is linked with lower HRV
The 2010 Biological Psychiatry meta-analysis found lower HRV in people with major depressive disorder compared with healthy controls. It also reported that tricyclic medication decreased HRV, while serotonin reuptake inhibitors, mirtazapine, and nefazodone did not show a significant HRV impact in that analysis.
The key practical point: if someone with depression has low HRV, it is not safe to assume the medication is the only driver. The underlying condition, sleep disruption, stress load, physical activity, and cardiovascular health may all be part of the signal.
Newer meta-analysis: SSRIs are still mixed
A 2023 systematic review and meta-analysis looked at antidepressant effects on autonomic nervous system outcomes, including HRV. It found that SSRIs were associated with lower RMSSD in randomized controlled trials, but higher RMSSD in pre-post studies. The authors described SSRI effects on many autonomic outcomes as no effect or inconclusive, depending on study design.
That is not a satisfying headline, but it is honest. SSRIs do not have a simple, universal HRV effect across all studies.
Tricyclic antidepressants show a clearer HRV drop
The strongest signal is for tricyclic antidepressants.
Older reviews and the 2023 meta-analysis both point toward TCAs reducing several HRV markers, especially parasympathetic markers. This makes sense pharmacologically because TCAs can have stronger anticholinergic and cardiovascular effects than most SSRIs.
That does not mean TCAs are never appropriate. It means HRV and heart-rate changes deserve more context, especially in people with cardiovascular risk, older adults, or anyone using a wearable to track recovery.
SNRIs and other antidepressants are less predictable
SNRIs such as venlafaxine and duloxetine may affect norepinephrine signaling, which can influence heart rate and blood pressure in some people. Bupropion, mirtazapine, trazodone, and newer agents have their own profiles.
The problem is that wearable users often ask, "What do antidepressants do to HRV?" That is too broad. The better question is, "What does this specific medication, at this dose, in this person, do to HRV over time?"
What You Might Notice on a Wearable
If you track HRV with Oura, Whoop, Garmin, Apple Watch, Polar, Fitbit, or another device, the first few weeks after starting or changing medication can look noisy.
A temporary HRV dip
Some people see a lower overnight HRV during the first days or weeks. That can happen if the medication affects sleep, appetite, hydration, GI comfort, or training routine.
A short-term dip is not automatically dangerous. It is a reason to zoom out and look at the trend.
A higher resting heart rate
If resting heart rate rises and HRV falls at the same time, the medication may be one possible contributor. But so could poor sleep, illness, alcohol, under-eating, dehydration, or higher emotional load.
The pattern matters more than a single night.
Better HRV as symptoms improve
Some people see HRV improve after anxiety calms down, sleep gets more consistent, panic symptoms reduce, or daily routines become easier. That improvement may reflect less overall stress, not a direct HRV-boosting effect from the drug itself.
A new baseline after dose changes
Dose increases, dose reductions, switching medications, or adding another medication can reset your wearable baseline. Give the data time before judging it. For most people, a few weeks of stable dosing gives a cleaner read than the first three nights after a change.
How to Interpret HRV While Taking an SSRI
The goal is not to ignore HRV. The goal is to stop overreading it.
1. Compare against your current baseline
Your pre-medication HRV is useful history, but it may not be the right comparison forever. Once your dose is stable, build a new baseline and watch deviations from that.
Ask:
- Is my 7-day or 30-day average changing?
- Did the change happen after a dose change?
- Did my sleep, alcohol intake, illness, training, or stress change too?
- Do I feel better, worse, or just different?
2. Track resting heart rate alongside HRV
HRV alone is too easy to misread. Pair it with resting heart rate, sleep duration, sleep regularity, symptoms, training load, and subjective mood.
If HRV falls but sleep improves, anxiety improves, and resting heart rate is stable, the meaning is different from a falling HRV paired with palpitations, insomnia, dizziness, or worsening exercise tolerance.
3. Do not use HRV to decide whether the medication is working
Antidepressant response is clinical. HRV is supportive context.
A higher HRV does not prove your SSRI is working. A lower HRV does not prove it is harming you. Mood, function, side effects, sleep, safety, and clinician follow-up matter more.
4. Watch for sustained changes, not one bad score
One ugly HRV reading is usually noise. A sustained shift over two to four weeks is more meaningful, especially if it lines up with symptoms or a medication change.
This is the same logic that applies to training recovery, illness, and sleep disruption. Trends beat single readings.
When to Talk With Your Clinician
A changed HRV trend alone is usually not an emergency. Symptoms matter more.
Talk with your clinician if you notice:
- persistent palpitations or a racing heartbeat
- dizziness, fainting, or unusual shortness of breath
- chest discomfort
- severe insomnia after starting or increasing a dose
- major fatigue that does not improve
- a resting heart rate that is clearly outside your normal range
- new exercise intolerance
- worsening mood, agitation, or suicidal thoughts
Do not stop, skip, or change antidepressant doses because of a wearable score. Some antidepressants need careful tapering, and abrupt changes can cause withdrawal symptoms or mood relapse.
Can You Support HRV While Taking Antidepressants?
Yes, but the boring basics matter more than trying to hack the number.
Protect sleep consistency
Sleep disruption can crush HRV, and some antidepressants can initially affect sleep. Keep wake time steady, reduce late-night light exposure, and avoid judging the medication from one rough night. If insomnia persists or you are consistently short on sleep, the guide to sleep deprivation and HRV gives useful context, but bring ongoing sleep problems up with your prescriber.
Keep alcohol low
Alcohol commonly lowers HRV and worsens sleep quality. If your HRV drops after starting medication but your drinking also increased, the wearable is not giving you a clean medication signal.
Train, but do not punish your nervous system
Exercise usually supports HRV over time, but hard training layered on poor sleep, appetite changes, or early medication side effects can backfire. Use easier aerobic work, walking, and light strength training when recovery is shaky.
Eat and hydrate consistently
Appetite changes are common with some medications and with depression itself. Under-fueling and dehydration can both drag HRV down. Keep meals, protein, fluids, and electrolytes boring and steady while your body adapts. For the food side, the broader nutrition and HRV guide is the better place to start than supplement experiments.
Use HRV as a conversation starter
If your HRV and resting heart rate changed after starting sertraline, escitalopram, fluoxetine, or another antidepressant, that is useful information. Bring the trend to your clinician with dates, dose changes, symptoms, and screenshots if needed.
A trend is much more useful than saying, "My recovery score is bad."
The Bottom Line
SSRIs can affect HRV, but the evidence is mixed and context-dependent. Depression and anxiety themselves are linked with lower HRV, SSRIs do not show one universal pattern, and tricyclic antidepressants have a clearer association with lower HRV markers.
If your wearable changes after starting an antidepressant, do not panic and do not ignore it. Look at the timing, dose, resting heart rate, sleep, symptoms, and longer trend. HRV can help you notice patterns, but medication decisions belong in a clinical conversation, not inside a recovery score.
Frequently Asked Questions
Do SSRIs lower HRV?
Sometimes, but not always. Research on SSRIs and HRV is mixed. Some studies find lower parasympathetic markers such as RMSSD, while others find little change or small improvements. The effect depends on the study design, medication, dose, diagnosis, and baseline health.
Does sertraline affect HRV?
Sertraline may affect HRV in some people, but there is no single expected wearable pattern. If your HRV changes after starting sertraline, compare it with resting heart rate, sleep, anxiety symptoms, alcohol intake, illness, and dose timing.
Does escitalopram lower HRV?
Escitalopram can change heart-rate and autonomic patterns in some users, but HRV changes are not predictable enough to use as a medication verdict. If you see a sustained HRV drop with symptoms like palpitations, dizziness, or severe insomnia, talk with your clinician.
Are tricyclic antidepressants worse for HRV than SSRIs?
In the research, tricyclic antidepressants have a clearer association with lower HRV and higher heart rate than SSRIs. That does not mean they are never appropriate, but it does mean HRV changes should be interpreted carefully, especially for people with cardiovascular risk.
Should I stop an antidepressant if my HRV drops?
No. Do not stop or change an antidepressant based on HRV alone. HRV is a useful trend marker, not a prescribing tool. Bring the trend, symptoms, and timing to your clinician before making any medication changes.
Need a quick read on your HRV number first?
Enter your HRV value, age range, device, and recovery context for a plain-English interpretation before you decide what to do next.
Interpret Your HRV NumberBuild the 30-day plan